


Estoy hablando de la campaña “Hands, de AT&T“, que fue un absoluto hit allá por el 2010, acumulando unos cuantos premios, entre ellos el de Mejor anuncio de revista favorito en EEUU.
¿Cómo llegamos a los distintos países? Esa fue la pregunta que se plantearon en BBDO Atlanta, la agencia publicitaria creadora de esta joya.
¿Cómo podemos mostrar la pluralidad del mundo, la cercanía de las personas y la tecnología todo a la vez?
Y nada, con un poco de imaginación y mucho mucho arte se pusieron manos a la obra, nunca mejor dicho.
El artista, el pintor que ha plasmado en las manos del modelo tantos lugares es Guido Daniele, reconocido body painter y el fotógrafo, Andric.
¿Cómo llegamos a los distintos países? Esa fue la pregunta que se plantearon en BBDO Atlanta, la agencia publicitaria creadora de esta joya.
¿Cómo podemos mostrar la pluralidad del mundo, la cercanía de las personas y la tecnología todo a la vez?
Y nada, con un poco de imaginación y mucho mucho arte se pusieron manos a la obra, nunca mejor dicho.
El artista, el pintor que ha plasmado en las manos del modelo tantos lugares es Guido Daniele, reconocido body painter y el fotógrafo, Andric.
La campaña, llamada AT&T Wireless International Roaming aunque se la conoce como “Hands by AT&T”, pretendía reflejar la conectividad de la compañía telefónica británica AT&T, gigante competencia de Movistar a nivel mundial y su fabuloso roaming en aquellos países en los que tenía presencia.
Os dejo unas cuantas muestras de los diferentes anuncios que se mostraron en algunos países:
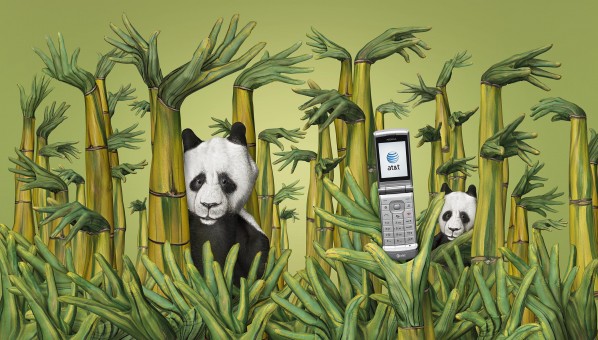
1. China
Un dragón, la gran muralla, osos panda… una China muy tradicional…

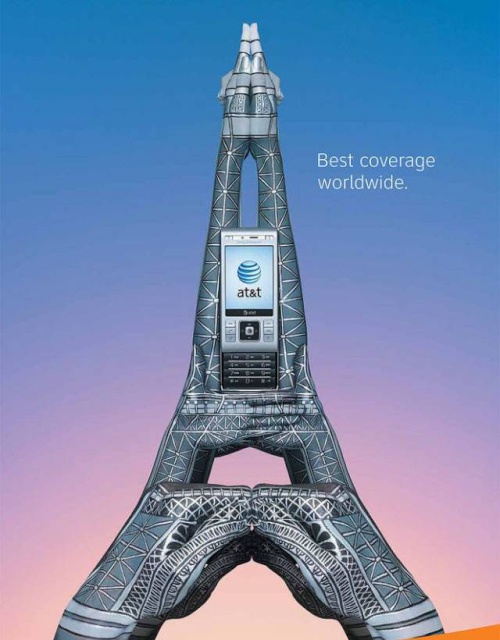
2. Francia
El símbolo francés por excelencia.
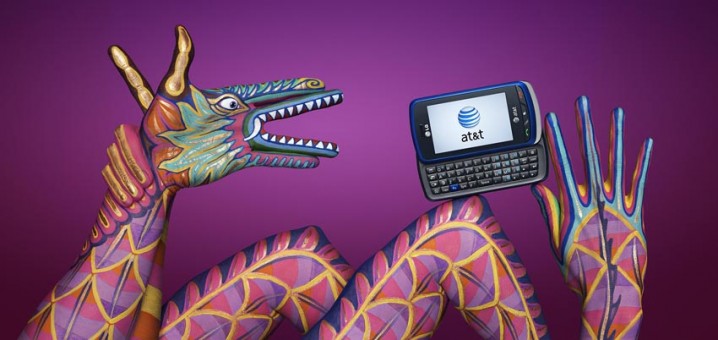
3. México
Unos chiles picantes y motivos mayas.





